West Coast Retina
Case of the Month
August, 2009
45 year old man with blurred vision, floaters and nyctalopia

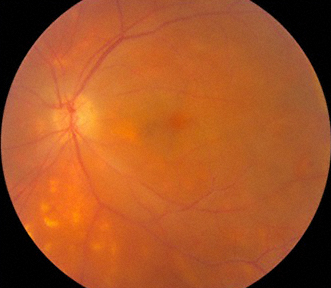
Figures 1: Color fundus photographs of the right and left eye. Note the media haze due to vitreous cells. Pale yellow-white oval lesions are scattered around the posterior pole
Case History
A 45-year-old man presented with a two month history of decreasing vision, floaters, and nyctalopia affecting both eyes. Past medical history was non-contributory. Best corrected visual acuity was 20/25 in each eye and intraocular pressures were within normal limits bilaterally. Examination of the anterior segment revealed 1+ cell and flare in the anterior chamber. Posterior segment examination demonstrated 2+ diffuse vitreous inflammation, mild disc edema, dilated retinal veins, and several yellow-white choroidal lesions in the mid- and far-periphery of each eye. (Figure 1) Bilateral leakage from the optic disc and retinal vessels was evident on fluorescein angiography. (Figure 2)
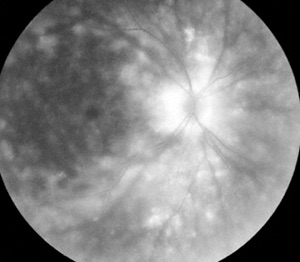
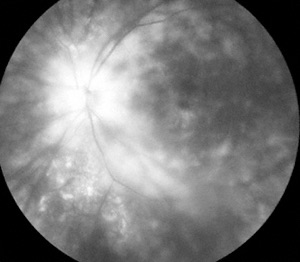
Figures 2: Late phase fluorescein angiogram of the right and left eye. Note the fluorescein staining of the nerve and the pale lesions. CME is present in both eyes.
What is your Diagnosis?
Differential Diagnosis
The most likely diagnoses for this patient included birdshot chorioretinopathy, syphilis, and sarcoidosis. Laboratory evaluations including serum FTA-ABS and RPR titers; serum ACE and lysozyme levels, and chest x-ray were normal. Also, antibody testing for HLA-A29 expression was negative.
Diagnosis
Because clinical suspicion of birdshot chorioretinopathy remained high, testing for HLA-A29 expression was repeated using a PCR-based method. This test revealed the presence of the HLA-A29 antigen, strongly suggesting the diagnosis of birdshot chorioretinopathy.
Discussion
Birdshot chorioretinopathy typically occurs in healthy patients in the 5th to 7th decade of life.1 Common symptoms include photopsia, nyctalopia, and dyschromatopsia. Findings on examination include vitritis as well as multiple bilateral and symmetrical cream colored lesions posterior to equator at the level of the choroid. Cystoid macular edema and retinal atrophy can, if untreated, result in decreased vision. Fluorescein angiography often reveals delay in the appearance of dye in the retinal arterioles as well as profuse vascular leakage associated with an increase in retinal circulation time.
The link between birdshot chorioretinopathy and HLA-A29 antigen expression has been firmly established.2,3 Reliable HLA-A29 subtyping is therefore vital in patients suspected of having birdshot chorioretinopathy.
The present report describes a patient with birdshot chorioretinopathy in whom initial antibody-based testing for HLA-A29 antigen expression was negative and in whom subsequent testing using a PCR-based technique was positive. Similar results have been reported for other HLA antigens.4-6 PCR-based testing should be considered when antibody-based testing for the HLA-A29 antigen is unexpectedly negative.7
Take Home Points
- Birdshot chorioretinopathy is characterized by multiple white-yellow flat, 500-1000 micron lesions.
- Age of onset is typically in the 5th to 7th decade of life, although occurrence in younger patients has been reported. Common symptoms are floaters, blurred vision and nyctalopia.
- Associated findings include vitreous cells, macular edema, and disc edema. Retina and optic nerve leakage are evident on fluorescein angiography.
- HLA-A29 positivity is strongly associated with this disorder.
- Sarcoidosis can mimic the findings of birdshot chorioretinopathy and should always be considered as part of the differential diagnosis.
- PCR testing can be very helpful in those cases when antibody testing is negative despite a high degree of clinical suspicion
Want to Subscribe to Case of the Month?
References
- Gass JD. Stereoscopic Atlas of Macular Diseases: Diagnosis and Treatment, 4th Ed. CV Mosby, June, 1999.
- Shah KH, Levinson RD, Yu F, et al. Birdshot chorioretinopathy. Surv Ophthalmol 2005;50:519-41.
- LeHoang P, Ozdemir N, Benhamou A, et al. HLA-A29.2 subtype associated with birdshot retinochoroidopathy. Am J Ophthalmol 1992;113:33-5.
- Schreuder GM, Hurley CK, Marsh SG, et al. HLA dictionary 2004: summary of HLA-A, -B, -C, -DRB1/3/4/5, -DQB1 alleles and their association with serologically defined HLA-A, -B, -C, -DR, and -DQ antigens. Hum Immunol 2005;66:170-210.
- Noreen HJ, Yu N, Setterholm M, et al. Validation of DNA-based HLA-A and HLA-B testing of volunteers for a bone marrow registry through parallel testing with serology. Tissue Antigens 2001;57:221-9.
- Kirveskari J, Kellner H, Wuorela M, et al. False-negative serological HLA-B27 typing results may be due to altered antigenic epitopes and can be detected by polymerase chain reaction. Br J Rheumatol 1997;36:185-9.
- Wender, JD, Fu AD, Jumper, JM, McDonald, HR, Johnson, RN, Cunningham, ET Jr: False negative antibody-based HLA-A29 typing in two patients with birdshot chorioretinopathy. Br J Ophthalmol. 2008 Aug;92(8):1153-4.