West Coast Retina
Case of the Month
August, 2011
Presented by Sandeep Randhawa, MD
A 77-year-old woman presented with blurred vision in her right eye for three weeks.


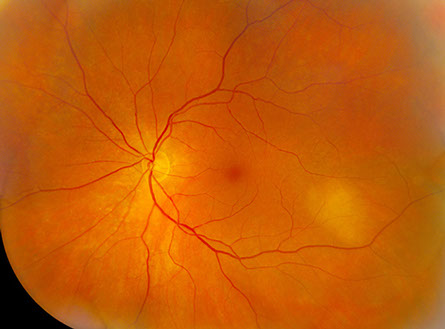
Figure 1: Color fundus photograph montages of the right and left eye. Note the two amelanotic choroidal lesions in the right eye and one amelanotic choroidal lesion in the left eye.
Case History
A 77-year-old woman presented with blurred vision in her right eye for three weeks and occasional photopsias. Her past medical history was significant for diabetes mellitus type 2, hyperlipidemia, hypertension, hypercholesterolemia, and osteoporosis. She was on exenatide injections, rosuvastatin, ezetimibe, lisinopril, and risedronate. She had a history of heavy smoking for a period of five years three decades ago.
On examination, her visual acuity was 20/125 in the right eye and 20/20 in the left. Intraocular pressures and slit lamp examination of the anterior segment were normal. Dilated fundus examination of the right eye (Figure 1) revealed two amelanotic slightly elevated choroidal lesions, one superior to the disc (measuring 6 mm vertically and 6 mm horizontally), and the other just inferior to the fovea (measuring 7 mm vertically and 8mm horizontally). Both lesions had surrounding subretinal fluid which extended to the macula. The left eye was also noted to have an amelanotic choroidal lesion just inferotemporal to the macula (no subretinal fluid was seen in the left eye).
What is your Diagnosis?
Differential Diagnosis
The differential diagnosis of circumscribed elevated amelanotic choroidal lesion includes amelanotic melanoma (and nevus), choroidal granuloma, choroidal hemangioma, choroidal lymphoma, choroidal metastases, and posterior scleritis.
Clinical Course
Further questioning revealed a remote history of breast cancer for which she had had a mastectomy thirty-four years prior to presentation, and had no evidence of recurrence.
Fluorescein angiography revealed early choroidal hypofluorescence along the lesions (with absence of vasculature) and progressive late hyperfluorescence from multiple pinpoint areas of leakage in the lesion (Figure 2). Optical coherence tomography revealed significant subretinal fluid with a hyperreflective and thickened retinal pigment epithelium-choriocapillaris complex (Figure 3). The ultrasound revealed an echogenic choroidal mass with high internal reflectivity (Figure 4). These findings were consistent with choroidal metastases.
The patient underwent a CT scan of her chest, abdomen, and pelvis as part a metastatic workup. The imaging revealed a focal mass in the right hilum extending to the right middle lobe, and diffuse pulmonary nodules (Figures 5A and 5B). There were also multiple lytic lucencies and blastic lesions throughout the bones consistent with osseous metastatic disease. The left lobe of the liver had an irregular mass concerning for a metastatic focus (Figure 6). The patient also had an MRI of the brain and orbits which was normal. She underwent a bronchoscopy with brush and endobronchial biopsy, which revealed a non-small cell carcinoma which was TTF (thyroid transcription factor) negative and estrogen receptor positive, consistent with breast carcinoma.1 The patient was treated with radiation therapy for the lung mass and systemic chemotherapy.
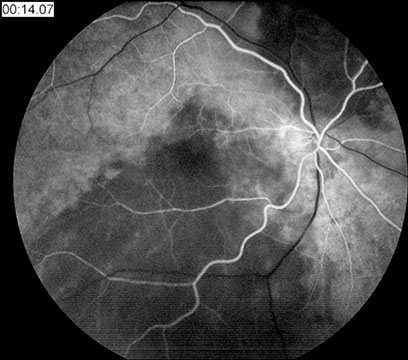
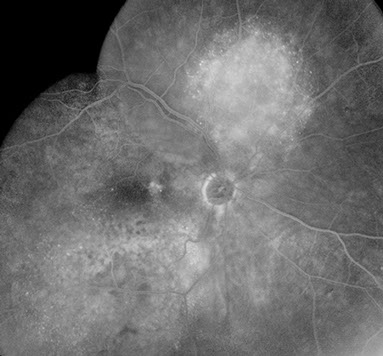
Figures 2: Fluorescein angiography revealed early choroidal hypofluorescence along the lesions (with absence of vasculature) and progressive late hyperfluorescence from multiple pinpoint areas of leakage in the lesion.

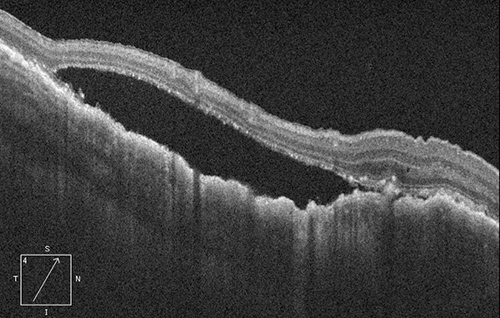
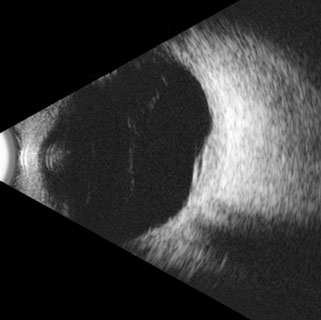
Figure 3: Spectral domain optical coherence tomography revealed significant subretinal fluid in the area of the lesion with a hyperreflective and thickened retinal pigment epithelium-choriocapillaris complex
Figure 4: The ultrasound reveals an echogenic choroidal mass with an overlying serous retinal detachment. The irregular contour and solid structure are diagnostic.

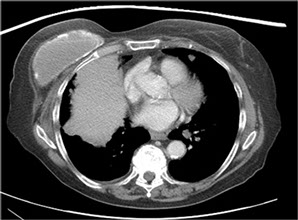

Figures 5: CT scan of the chest revealing a focal mass in the right hilum extending to the right middle lobe.
Figure 6: CT of the abdomen showing an irregular mass in the left lobe of the liver concerning for a metastatic focus.
Discussion
Uveal metastasis is considered to be the most frequent intraocular malignancy, with an estimated annual incidence of 20,000 patients in the United States. Breast carcinoma is the most common cancer to affect women in the United States with one in eight women anticipated to develop this malignancy over a lifetime.2
Breast cancer is also the most common malignancy to metastasize to the uvea.3 It accounts for 40% of all uveal metastasis.4 Shields et al in their series of 520 patients with uveal metastases found that the most common primary tumor site was breast (47%), followed by lung (21%), and gastrointestinal tract (4%).3 Kamby et al reported that breast cancer has an overall metastatic rate of 23% at a median follow-up of 4.9 years. The five most common sites of metastasis include lung (71%), bone (71%), lymph nodes (67%), liver (62%), and pleura (50%).5
Choroidal metastasis is the smallest detectable lesion of metastatic breast cancer and was detected at a median of 3 years after diagnosis of the primary cancer.6
A striking majority of choroidal metastases from breast cancer are yellow in color, plateau shaped, associated with subretinal fluid, and located posterior to the equator.7 Choroidal metastases from breast cancer was more commonly bilateral (33%) and multifocal (32%) compared with other primary neoplasms.4 The B-scan ultrasound shows an echogenic subretinal mass with diffuse, ill-defined borders and the A-scan demonstrates moderate to high internal reflectivity.8
Ocular metastasis from breast cancer typically develops after the diagnosis of the primary cancer and after other systemic metastasis has been detected. Clinical studies show that choroidal metastasis in breast cancer occurs predominantly in patients in whom systemic metastases involve more than one organ system, resulting in a risk of developing ocular metastasis of approximately 11% in these patients.9 Ocular metastasis can sometimes be the initial manifestation of breast cancer. In some studies, ocular metastasis from breast cancer was the presenting sign in 4% to 46% of patients or the initial site of systemic dissemination in 12% to 31% of patients with breast cancer.4,6,9,10
Our case is unique because the choroidal metastases occurred after a disease-free period of thirty four years, the longest reported in the literature.
Take Home Points
- Cancer metastasis to the uvea is by far the most frequent intraocular tumor. Aided by slit lamp biomicroscopy, uveal metastasis is the smallest detectable breast cancer metastasis in the human body. Lesions as small as 1 mm can be detected. The detection of such early metastasis in the eye can signal the need for systemic evaluation.
- Even though metastasis from breast cancer typically develops after the diagnosis of the primary site and after systemic metastases has occurred, it may often be the presenting sign of systemic metastases. This underscores the importance of routine ocular examination for all patients and especially those with breast cancer.
- In rare cases, the metastases from primary breast cancer may occur after a very long period of remission.
Want to Subscribe to Case of the Month?
References
- Vollmer RT. Primary lung cancer vs metastatic breast cancer: a probabilistic approach. Am J Clin Pathol 2009 Sep;132(3):391-5.
- Lantz PM, Booth KM. The social construction of the breast cancer epidemic. Soc Sci Med 1998;46:907-918.
- Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE. Survey of 520 eyes with uveal metastases. Ophthalmology 1997;104:1265–1276.
- Ferry AP, Font RL. Carcinoma metastatic to the eye and orbit. I. A clinicopathologic study of 227 cases. Arch Ophthalmol 1974;92:276–286.
- Kamby C, Ejlertsen B, Andersen J, et al. The pattern of metastases in human breast cancer: Influence of systemic adjuvant therapy and impact on survival. Acta Oncologica 1988;27:715-719.
- Mewis L, Young SE. Breast carcinoma metastatic to the eye: Analysis of 67 patients. Ophthalmology 1982;89:147-151.
- Demirci H, Shields CL, Chao AN, Shields JA. Uveal metastasis from breast cancer in 264 patients. Am J Ophthalmol 2003 Aug;136(2):264-71.
- Shammas HJ. Atlas of ophthalmic ultrasonography and biometry. St Louis: Mosby; 1984.
- Wiegel T, Kreusel KM, Bornfeld N, et al. Frequency of asymptomatic choroidal metastasis in patients with disseminated breast cancer: results of a prospective screening programme. Br J Ophthalmol 1998; 82:1159–1161.
- Merrill CF, Kaufman DI, Dimitrov NV. Breast cancer metastatic to the eye is a common entity. Cancer 1991;68:623–627.