West Coast Retina
Case of the Month
August, 2012
A 18-year-old woman with blank spots in the vision of her left eye.
Presented by Sara Haug, MD, PhD

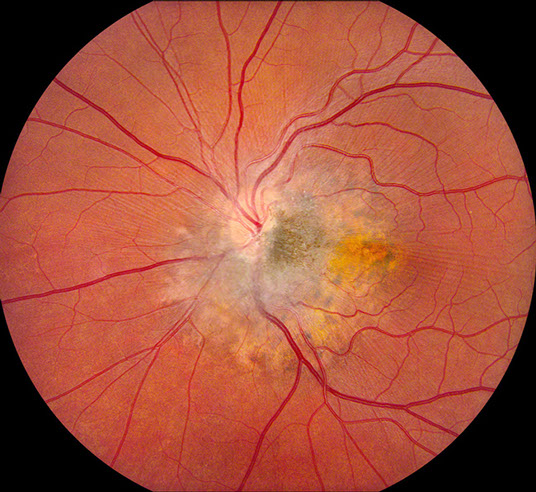
Figure 1: Fundus photograph of the left eye showing an irregular leopard-spotted lesion with central hyperpigmentation at the optic nerve temporal border. Subtle retinal striae emanating from the lesion are observed.
Case History
An 18 year-old-woman presented for evaluation of a lesion on the fundus of her left eye. The patient noted seeing “blank spots” in her left eye since at least 2008. Medical history and review of systems were otherwise normal. On examination, vision was 20/16 OD, 20/50 OD. Intraocular pressures were 15 OD, 12 OS.
Examination of the right eye was entirely normal. Funduscopic examination of the left eye showed a leopard-spotted lesion with peripapillary hyperpigmentation and scalloped borders (Fig 1). Islands of RPE hyperpigmentation are observed at the periphery of the lesion. Some areas of fibroglial tissue are noted overlying the lesion resulting in subtle retinal striae extending from the lesion into the macula.
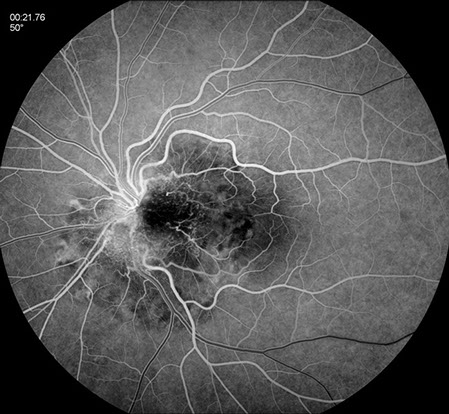
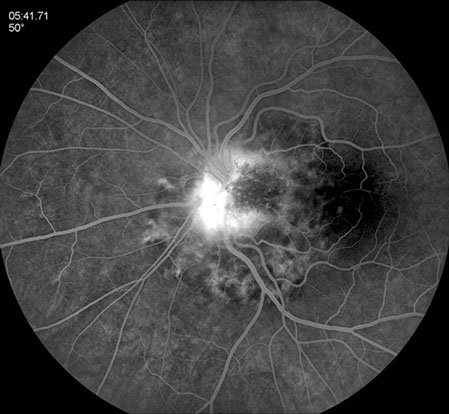
The fluorescein angiogram shows early blockage temporally with irregular central hyperfluorescence and staining and retinal vascular tortuosity (Fig 2A). The late angiogram demonstrates intense hyperfluorescent leakage associated with glial membrane traction (Fig 2B). The lesion appears dark on fundus autofluorescence (Fig 3 and 4B).
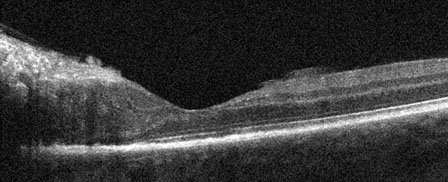
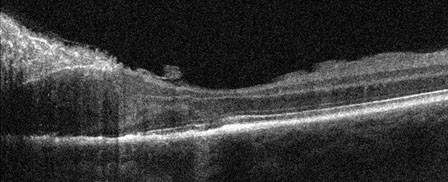
SD-OCT through the fovea shows loss of normal retinal architecture in the area of the lesion with marked hyperreflective glial proliferation (Fig 5A and B). The adjacent retina has retinal pigment epithelium irregularities including areas of hypertrophy and atrophy. There is also mild disruption of the IS/OS junction.
A
B
Figures 2A and B: Fluorescein angiogram left eye. There is early blockage with some areas of increasing fluorescence. Central hyperfluorescence is seen in the late phase of the angiogram. Note the scalloped pattern of fluorescence, most apparent in the nasal and inferior portion of the lesion.
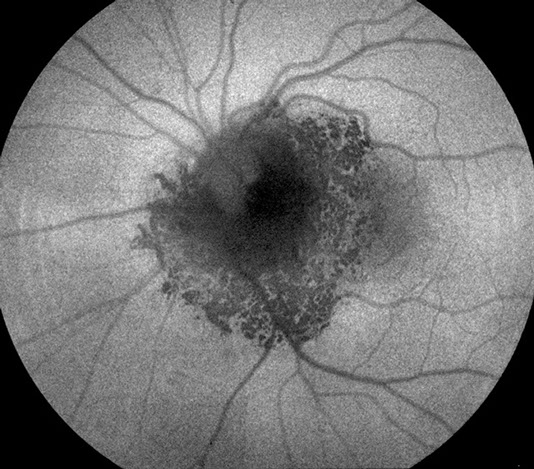
Figure 3: Fundus autofluorescence image of the left eye. The lesion mostly shows reduced autofluorescence, but in the areas of the scalloped borders, there is normal to increased autofluorescence.
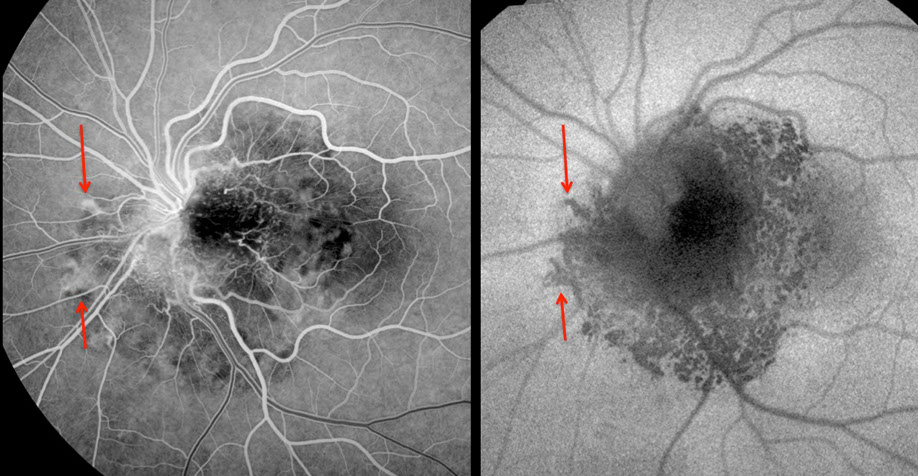
Figure 4: Early fluorescein angiogram on the left and autofluorescence image on the right. The arrows indicate corresponding regions and demonstrate the inverted fluorescence pattern that is typical of this entity.
A
B
Figures 5A and B: Horizontal SD-OCT scans of the left eye through the lesion and macula. Note the disorganization of the retinal layers through the lesion. Within the lesion, there is irregularity of the photoreceptors and the retinal pigment epithelium although the fovea is largely preserved (A).
What is your Diagnosis?
Differential Diagnosis
Degenerations
Pseudoxanthoma Elasticum
Dystrophy
Sjogren’s Reticular Dystrophy
Infectious
Syphilis
Inflammatory
Posterior Scleritis
Harada’s Disease
Immunologic
Bilateral Diffuse Uveal Melanocytic Proliferation
Iatrogenic
Phototoxicity
Idiopathic
Uveal Effusion Syndrome
Central Serous Retinopathy
Tumor
Lymphoma
Leukemia
Choroidal Osteoma
Metastasis
RPE Adenoma
Benign Reactive Lymphoid Hyperplasia
Choroidal Hemangioma
Combined Retina-RPE Hamartoma
Toxicity
Thioridazine
Trauma
Hematologic
Thrombotic Thrombocytopenic Purpura
Hereditary
Sector Retinitis Pigmentosa
Congenital
Unilateral Retinal Pigment Epithelium Dysgenesis
Congenital Hypertrophy of the RPE
Discussion
The appearance and characteristic fluorescein angiogram and fundus autofluorescence findings are consistent with a diagnosis of unilateral retinal pigment epithelium dysgenesis (URPED). Nine cases of URPED have been described in the literature.1,2 Although there is variability in the appearance of the lesions, Cohen et al. describe two defining characteristics.1 First, the scalloped atrophic border of the lesion with islands of RPE hyperplasia is considered pathognomic. Second, the inverted pattern of FAF and FA is another characteristic finding for URPED.1 The fundus autofluorescence image reveals, areas of reduced autofluorescence that correspond to areas of hyperfluorescence on the fluorescein angiogram, whereas areas of hypofluorescence on the angiogram show normal to slight increased autofluorescence.
Combined hamartoma of the retina and retinal pigment epithelium needs to be considered in the differential diagnosis of our case. Combined hamartomas are characterized by hyperpigmentation of the RPE, retinal vascular tortuosity, and glial proliferation and have a characteristic pattern of punctate hyperfluorescence resembling a “starry night”.3,4 In almost all ways, our case could be a routine combined hamartoma of the retina and RPE. However, the distinguishing feature of unilateral RPE dysgenesis is the characteristic scalloped border of the RPE. This case has a classic border pattern of URPED.
So, what is the diagnosis? The RPE border of our lesion fits well within the definition of URPED. Indeed, several of the original cases describing this entity also have classic features of combined hamartomas. It is probable that “unilateral RPE dysgenesis” and “combined hamartomas of the retina and RPE” are disorders on opposite ends of the same clinical spectrum.
URPED lesions may enlarge with time and also may be associated with retinal folds, vascular tortuosity, and CNV. In the largest series of URPED to date, visual prognosis was good although follow-up limited.1
Take Home Points
- Defining characteristics of unilateral retinal pigment epithelium dysgenesis include a scalloped fringe of fibrosis and atrophy with islands of hyperplastic RPE as well as a distinct inverted pattern on fundus autofluorescence and fluorescein angiogram.
- Some cases of URPED have glial proliferation and retinal vascular tortuosity identical to that found in combined retinal-RPE hamartoma.
- The visual prognosis is largely thought to be good, although subfoveal CNV can lead to decrease in vision.
Want to Subscribe to Case of the Month?
References
- Cohen SY, Fung AE, Tadayoni R et al. Unilateral Retinal Pigment Epithelium Dysgenesis. Am J Ophthalmol 2009;148:914-9.
- Cohen SY, Massin P, Quentel G. Unilateral, idiopathic leopard-spot lesion of the retinal pigment epithelium. Arch Ophthalmol 2002;120:512-6.
- Gass JD. An unusual hamartoma of the pigment epithelium and retina simulating choroidal melanoma and retinoblastoma. Trans Am Ophthalmol Soc 1973;1:175-83.
- Shields CL, Thagnappan A, Hartzell K et al. Combined hamartoma of the retina and retinal pigment epithlium in 77 consecutive patients. Ophthalmol 2008;115:2246-52.