West Coast Retina
Case of the Month
November, 2011
Presented by Paul Stewart, MD
A 26-year-old man with blurred vision and multiple scotoma in both eyes.

A
B
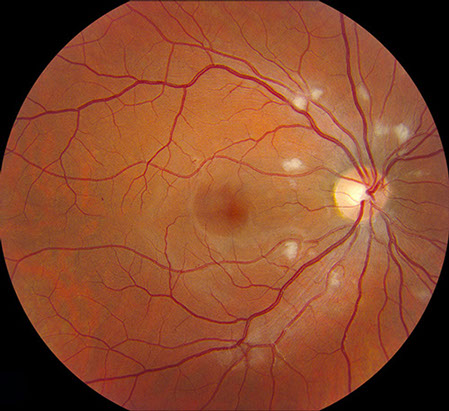
Figures 1A and B: Fundus photograph of the right and left eye. Note the multiple cotton-wool spots scattered around the disc of each eye. A few microaneurysms are present in the right eye and a small intraretinal hemorrhage is seen just nasal to the left optic nerve (arrow).
Case History
A 26-year-old man described blurred vision and multiple scotomata in both eyes which developed 2 weeks prior to a hospitalization for acute pancreatitis secondary to alcohol abuse. He had a 20-year history of type 1 diabetes. During his 4-day hospital stay, he was treated with IV fluids and potassium supplements. He had no other past medical or ocular history.
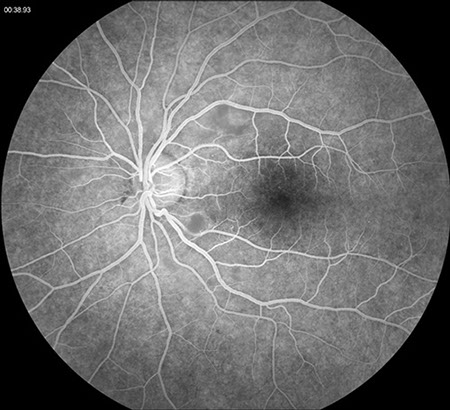
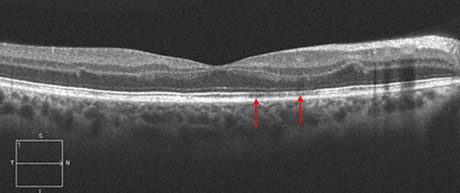
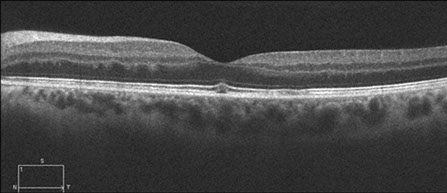
On examination, best-corrected visual acuity was 20/160 in the right eye and 20/100 in the left eye. Intraocular pressures ware 17 mmHg bilaterally. He had scattered defects on Amsler grid testing in both eyes, but both visual fields were otherwise full to confrontation. Anterior segment examination was unremarkable in both eyes. Fundus examination of the right eye showed several microaneurysms and multiple cotton-wool spots surrounding the optic nerve. There was no optic nerve swelling. (Figure 1A) Fundus examination of the left eye showed similar circumpapillary cotton-wool spots with a single intraretinal hemorrhage adjacent to the disc (Figure 1B). Fluorescein angiography showed the cotton wool spots, but did not reveal retinal or choroidal ischemia. (Figures 2). Optical coherence tomography revealed a normal foveal contour with possible inner segment/outer segment (IS/OS) junction attentuation (Figure 3A) and a normal foveal contour with a small amount of subfoveal fluid in the left eye (Figure 3B).

A
B
Figures 2A and B: Fluorescein angiogram of the right and left eye. Normal and timely filling the retinal vessels was present with no evidence of retinal or choroidal ischemia. Later phase angiograms (not shown), did not demonstrate retinal vascular or optic disc leakage.
A
B
Figures 3A and B: Spectral domain optical coherence tomography of the right (A) and left (B) macula. The IS/OS junction in the right eye shows attenuation (arrows). In the left eye, a small amount of subfoveal fluid is present.
What is your Diagnosis?
Differential Diagnosis: Circumpapillary Cotton Wool Spots
- Acute pancreatitis
- Diabetic retinopathy
- Hypertensive retinopathy
- Radiation retinopathy
- Interferon retinopathy
- HIV retinopathy
- Long bone fracture/orthopedic surgery
- Chest compression injuries
- Chronic renal failure
- Hemolytic uremic syndrome
- Childbirth
- Connective tissue disorders; most commonly systemic lupus erythematosus
- Cryoglobulinemia
- Weight-lifting
- Shaken baby syndrome
- Retrobulbar and periocular injections
- Valsalva maneuver
- Commotio retinae
- Multiple myeloma
Clinical Course
Two weeks following the initial evaluation, his vision had improved to 20/25 in the right eye and 20/32 in the left eye.
Discussion
Purtscher first described the condition that bears his name in 1910 in a patient with head trauma from a fall. He described areas of bilateral retinal whitening and hemorrhage. Vision recovered without treatment.
The vision loss associated with Purtscher’s retinopathy typically occurs within a day or two of the insult, and can range from minimal to profound.. Scotomata are common and may be central, paracentral or arcuate. The cotton wool spots of Purtscher's retinopathy, also known as Purtscher flecken, cluster around the disc and are typically found between the retinal venules and arterioles – with a characteristic clear zone observed adjacent to the arterioles. In addition to cotton wool spots, fundus examination can reveal intraretinal hemorrhages, optic disc swelling, and, in severe cases, a cherry red spot.
Fluroescein angiography and indocyanine green angiography typically show variable degrees of retinal and choroidal non-perfusion, respectively. Optical coherence tomography can show both swelling of the nerve fiber layer and disruption of the IS/OS junction, as observed in our case.
The exact pathogenesis of the retinal findings observed in Purtscher’s retinopathy is unknown, but is believed to involve embolic occlusion of the precapillary arterioles, which measure approximately 50 microns in diameter. Potential emboli include air, fat, leukocyte aggregates, platelets and fibrin, depending on the inciting factor. It has been postulated that intravascular lipase and complement activation might promote local leukocyte aggregation, thus further promoting small vessel occlusion.
Vision recovery varies and appears to depend most directly on the degree and extent of retinal and choroidal non-perfusion. High dose intravenous corticosteroids have been used in the acute setting with variable results. Plasmapheresis has been suggested to be effective in selected patients with active systemic vasculitis, most notably systemic lupus erythematosus.
Take Home Points
- The vision loss associated with Purtscher’s retinopathy tends to occur within a day or two of the insult and is variable, depending most directly upon the degree and extent of retinal and choroidal non-perfusion.
- The pathogenesis of Purtscher’s retinopathy involves occlusion of retinal precapillary arteriole(s).
- A Purtscher-like retinopathy can be associated with a number of systemic conditions, including acute pancreatitis.
Want to Subscribe to Case of the Month?
References
- Agrawal A and McKibbin MA. “Purtscher’s and Purtscher-like Retinopathies: A Review,” Survey of Ophthalmology. 51:2, 2006, 129-136.
- Burton TC. “Unilateral Purtscher’s retinopathy,” Ophthalmology. 87, 1980, 1096-1105.
- Wang AG, Yen MY, Liu JH. “Pathogenesis and neuroprotective treatment in Purtscher’s retinopathy,” Jpn J Ophthalmol. 42, 1988, 318-322.
- Beckingsale AB, Rosenthal AR. “Early fundus fluorescein angiographic findings and sequelae in traumatic retinopathy: a case report,” Br J Ophthalmol. 67, 1983, 119-123
- Gomez-Ulla F, Fente B, Torreiro MG, et al. “Choroidal vascular abnormality in Purtscher’s retinopathy shown by indocyanine green angiography,” Am J Ophthalmol. 122, 1996, 261-263.
- Behrens-Baumann W, Scheurer G, Schroer H. “Pathogenesis of Purtscher’s retinapathy. An experimental study,” Graefes Arch Clin Exp Ophthalmol, 230, 1992, 286-291
- Harrison TJ, Abbasi CO, Khraishi TA. “Purtscher retinopathy: an alternative etiology supported by computer fluid dynamic simulations,” Invest Ophthalmol Vis Sci. 52: 11, 2011, 8102-8107.
- Atabay C, Kansu T, Nurlu G. “Late visual recovery after intravenous methylprednisolone treatment of Purtscher’s retinopathy,” Ann Ophthalmol. 25, 1993, 330-333.
- Hollo G, Tarjanyi M, Varga M, et al. “Retinopathy of pancreatitis indicates multiple-organ failure and poor prognosis in severe acute pancreatitis,” Acta Ophthalmol. 72, 1994, 114-117.
- Shein, J, Shukla D, Reddy S, Yannuzzi LA, Cunningham ET Jr. Macular infarction as a presenting sign of systemic lupus erythematosus. Retina Cases & Case Series 2008, 2:55-60.