West Coast Retina
Case of the Month
October, 2010
Presented by Jon Wender, MD
A 4-year-old boy was referred for an asymptomatic macular lesion in the left eye.
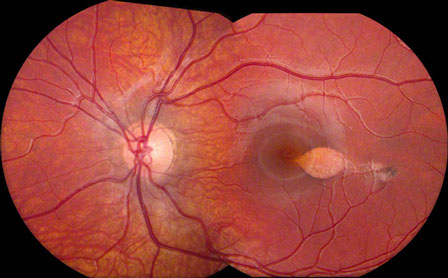
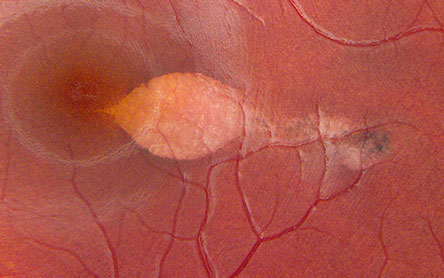
Figures 1: Color montage of the left eye and detail of lesion. Note the oval-shaped lesion at the temporal edge of the fovea. The edges of the lesion show subtle hyperpigmentation, and there is a trailing edge extending temporally.
Case History
A 4-year-old boy without any visual complaints was referred from the pediatric ophthalmologist for a macular lesion in the left eye. His past ocular and medical history were unremarkable and he was not taking any medications. He was born to a healthy mother at 38 weeks gestational age with a birth weight of 6 pounds, 14 ounces. His family history was significant for a sister with accommodative esotropia as well as an aunt and a niece with decreased vision of unclear etiology.
On examination, the visual acuity was found to be 20/20 in each eye. The anterior segment examination was normal in each eye. The dilated fundus examination was normal in the right eye. In the left eye, there was an oval-shaped, flat, hypopigmented macular lesion with surrounding hyperpigmentation and a tip pointing towards the fovea (Figure 1). Optical coherence tomography (OCT) of the left eye revealed a normal vitreoretinal interface, normal foveal contour, the absence of intraretinal or subretinal fluid, and attenuated retinal pigment epithelium (RPE) in the region of the hypopigmented macular lesion (Figure 2). Three months after the initial presentation, the patient was still asymptomatic, the visual acuity was unchanged, and the macular lesion was stable.
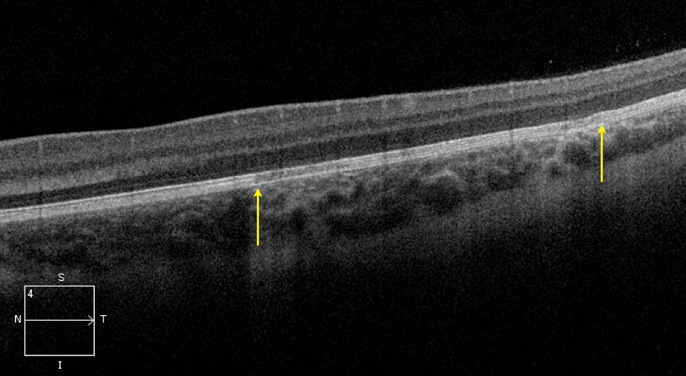
Figure 2: A horizontal scan spectral domain OCT scan through the lesion. Note the area of RPE attenuation (arrows). This lesion does not demonstrate the overlying cleft that has been reported in other similar lesions.
What is your Diagnosis?
Differential Diagnosis
The differential diagnosis for this lesion includes congenital albinotic spot of the retinal pigment epithelium (RPE), congenital hypertrophy of the RPE (CHRPE), and an inactive inflammatory chorioretinal scar. The clinical features, however, are most consistent with torpedo maculopathy.
Discussion
In 1992, Roseman and Gass used the term “solitary hypopigmented nevus of the RPE” to describe an atrophic macular lesion with a tail pointing towards the fovea in a 12-year-old boy.1 The name “torpedo maculopathy” was first used by Daily in 1993 to depict a lesion with a similar appearance to that described by Roseman.2
Patients with torpedo maculopathy are typically asymptomatic and have normal vision.3 It is most often diagnosed in young patients. Characteristic morphologic features include a location temporal to the fovea, sparing of the foveal center, and a tip that points towards the center of the macula. The lesion itself tends to be hypopigmented with sharply demarcated and hyperpigmented borders.1 The lesion usually remains stable in size and appearance over time.3
Ancillary testing, including fluorescein angiography (FA), fundus autofluorescence (FAF), OCT, and Humphrey visual field (HVF) testing, may demonstrate characteristic features in torpedo maculopathy. Hyperfluorescence secondary to window defect in the area of the lesion may be evident with FA and the lesion may cause hypoautofluorescence as revealed by FAF imaging. Optical coherence tomography typically reveals an abnormal and diminished RPE signal as well as a subretinal cleft that corresponds with the lesion.3 A visual field defect that correlates with the region of the macular lesion may also be present. Although previously referred to as nevi,1 several features, including hypoautofluorescence, RPE hyporeflectivity, and HVF scotomata, suggest that these lesions actually represent dysfunctional or absent RPE.3
Take Home Points
- Torpedo maculopathy is typically an asymptomatic lesion that has characteristic ophthalmoscopic features, including intrinsic hypopigmentation and a tail that points towards the center of the fovea.
- The lesion does not impair visual acuity and it tends to remain stable over time.
- Evaluation with OCT imaging, HVF testing, and FAF suggest that these lesions represent absent or abnormal RPE rather than nevi.
Want to Subscribe to Case of the Month?
References
- Roseman RL, Gass JD. Solitary hypopigmented nevus of the retinal pigment epithelium in the macula. Arch Ophthalmol 1992;110(10):1358-9.
- Daily MJ. Torpedo maculopathy or paramacular spot syndrome. New Dimensions in Retina Symposium. Chicago, 1993.
- Golchet PR, Jampol LM, Mathura JR, Jr., Daily MJ. Torpedo maculopathy. Br J Ophthalmol;94(3):302-6.