January, 2023
Presented by Presented by Georgia Kamboj, MD, PhD


Presented by Presented by Georgia Kamboj, MD, PhD
A 74-year-old white woman was referred with hyperpigmented lesions in the left eye.

Figure 1: Color photo montage of the right eye. Note the hyperpigmented cluster of spots in the inferonasal retina.
The patient was referred after a routine examination found some pigmented spots in her retina. She denied changes to her vision, flashes/floaters, metamorphopsia, and photophobia. Her past ocular history was positive for hyperopia. Past medical history was significant for oral lichen planus and hypercholesterolemia. She had no personal or family history of malignancy. Review of systems was negative.
The patient’s best corrected Snellen visual acuity measured 20/25 in each eye. Intraocular pressure was normal in both eyes. Anterior segment exam revealed nuclear sclerotic cataracts in both eyes. Posterior segment exam of the right eye was unremarkable. The left fundus was significant for scattered, deep, pigmented spots in the inferonasal quadrant (Figure 1). The vasculature appeared normal and there was no macular edema. Macular optical coherence tomography (OCT) of both eyes was unremarkable. OCT taken through one of the pigmented lesions in the left eye showed normal retinal and choroidal layers (Figure 2).
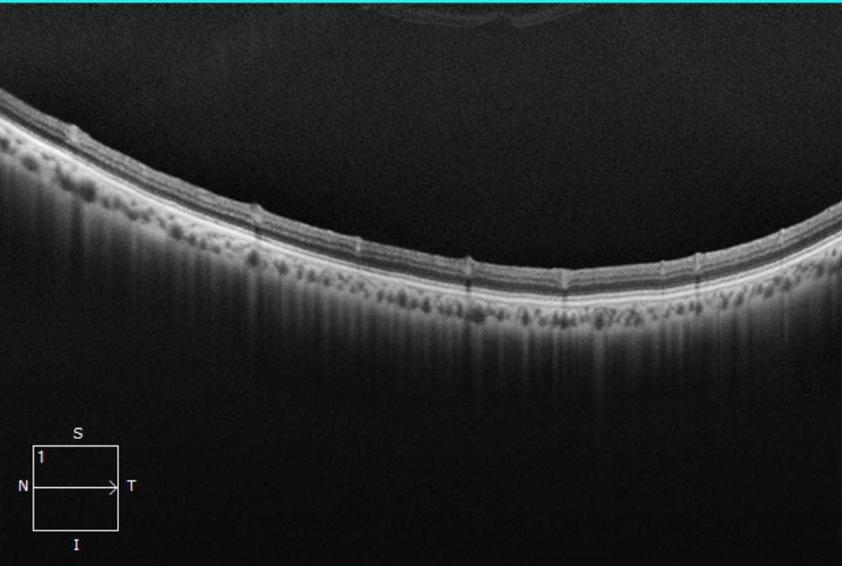
Figure 2:OCT-SD of the left eye through one of the pigmented lesions. The scan is unremarkable in this area.
She has had regular colonoscopies for cancer screening as recommended for her age. Colonoscopies have been negative for colon cancer and colonic polyps.
Differential Diagnosis
A diagnosis of grouped CHRPE (bear tracks) was made based on the distribution of pigmented fundus lesions and appearance on multimodal imaging. There was no concern for a systemically associated syndrome given that the lesions were unilateral and the patient’s medical and family history were negative. Observation of the lesions without further workup was recommended.
Discussion
Congenital Hypertrophy of the Retinal Pigment Epithelium (CHRPE) is a congenital hamartoma of the RPE. Asymptomatic, single or grouped pigmented fundus lesions are most commonly seen at presentation. Rarely, extension to involve the fovea can result in visual impairment.1 Lesions can be classified into three distinct categories; solitary CHRPE, multifocal grouped CHRPEs (also known as bear tracks), and grouped CHRPEs with systemic association. CHRPEs have been noted to enlarge over time.2
CHRPEs are typically benign except in rare circumstances when associated with familial adenomatous polyposis (FAP) syndromes. There are also reports of nodular pigmented adenocarcinomas arising from within areas of CHRPE causing CME or serous retinal detachment.3 On histopathology, benign CHRPEs are characterised by a layer of hypertrophied RPE cells, thickened Bruch’s membrane and photoreceptor degeneration with gliosis corresponding to depigmented lacunae.4 The choroid, choriocapillaris and inner retinal layers are unaffected. Atypical CHRPE lesions associated with FAP show RPE hypertrophy and hyperplasia, retinal invasion and retinal vascular changes.5
Characteristic features on examination and on imaging can help to differentiate between benign and systemically associated lesions clinically. Solitary CHRPEs present as flat, hyperpigmented lesions, with or without lacunae, located at the equatorial region.6 On fundus autofluorescence, lesions appear hypoautofluorescence with few areas of iso or hyper autofluorescence. OCT through lesions shows thickening of the RPE with overlying outer retinal atrophy. Multifocal grouped lesions (bear tracks) appear as multiple, small flat pigmented lesions located at the posterior pole and gradually increasing in number towards the periphery. Importantly, benign grouped lesions are usually seen unilaterally and within one quadrant of the retina. OCT through these lesions often appears normal. Features concerning for systemically associated cancer syndromes include bilaterality, distribution across the fundus, irregular margins or spindle shaped, depigmented halos around the lesions and the appearance of retinal vasculature abnormalities overlying lacunae.6,7 These lesions often show thickening and intraretinal extension of the RPE layer hypertrophy with outer retinal atrophy on OCT.